2026 Prescriptive Authority Rules Every NP Student Should Understand
Co-Founder and Chief Data Scientist
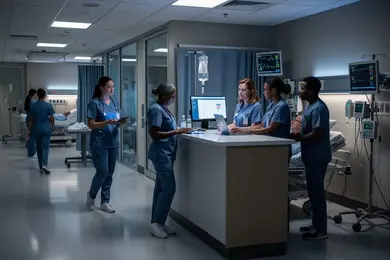
Imagine a nurse practitioner student navigating the rapidly changing landscape of prescriptive authority without clear, up-to-date guidance-facing state-by-state regulatory shifts that directly influence clinical autonomy and employment prospects. Nearly 65% of graduate nursing learners now enroll in part-time or online nurse practitioner programs, according to the National Center for Education Statistics, reflecting growing demand for flexible pathways amid workforce shortages.
This shift intensifies the need for precise understanding of prescriptive limits, especially as scope of practice laws remain a patchwork. This article clarifies prescriptive authority rules, enabling NP program students to anticipate legal boundaries, optimize clinical choices, and align education with career strategies effectively.
Key Things You Should Know
- State-specific prescriptive authority scope varies broadly, with 28 states granting full authority, but restrictive protocols and delayed DEA registration requirements extend employment start by 3-6 months in 44% of cases, per 2024 Nursing Workforce Survey.
- Employers increasingly require dual certification in both acute and primary care specialties, with 62% of surveyed health systems favoring such versatility, raising costs by 15-25% for additional NP Programs credentials within two years.
- The growing Medicaid reimbursement differential-up to 20% less for NPs in certain states-forces graduates to weigh immediate salary compromises against long-term autonomy gains, complicating decisions on costly NP Programs investments.
What is prescriptive authority for nurse practitioners and why does it matter?
Prescriptive authority regulations for nurse practitioners in the US create tangible divisions in practice autonomy that shape workforce dynamics and educational design. Currently, 29 states, the District of Columbia, and two territories grant full prescriptive authority, allowing NPs to prescribe medications-including controlled substances-without mandatory physician oversight.
This enables independent management of chronic and urgent care treatments in outpatient and specialty settings, reducing bottlenecks seen in states with more restrictive collaborative agreements. For employers, jurisdictions with full authority experience faster hiring and prioritize candidates trained under broader scopes, directly affecting labor market competitiveness.
The importance of prescriptive authority in nurse practitioner education becomes evident when comparing program outcomes by state. Students targeting full authority regions engage in richer clinical experiences with direct pharmacologic management, enhancing readiness for independent practice. Conversely, programs in restrictive states emphasize compliance with limits on prescribing, which narrows practical exposure and may constrain long-term flexibility.
These regulatory nuances inform not only curricular focus but also influence career trajectory and salary potential. Working professionals should strategically assess these regulations for relocation or credentialing decisions, especially when pursuing niche qualifications such as acute care nurse practitioner certification. Understanding the legal framework around prescriptive authority is integral to negotiating clinical privileges and aligning with evolving hiring priorities across state lines.
How do nurse practitioner prescriptive authority rules differ by state?
Nurse practitioner prescriptive authority rules vary widely across states, shaping both the scope and autonomy of NP practice. As of September 2025, 28 states plus the District of Columbia grant full prescriptive authority, enabling NPs to prescribe independently without physician oversight. This contrasts sharply with states imposing reduced or restricted authority, where formal collaborative agreements or direct physician supervision are mandatory.
Such variation affects clinical workflows and hiring dynamics, particularly in rural or primary care settings where independent prescribing expedites patient management. State-specific nurse practitioner prescription regulations demand strategic consideration by prospective NPs. In full-authority states, the ability to open private practices or work with minimal oversight can enhance employment opportunities and reduce administrative complexity.
Meanwhile, restricted states require ongoing physician collaboration, which can delay medication management and limit roles within telehealth or specialties demanding quick adjustments. Employers in restricted jurisdictions often prefer candidates with established collaborative agreements, adding layers of administrative and contractual complexity. Consequently, students should prioritize understanding these variations during their education, focusing on relevant clinical hours and coursework aligned with their target states.
Variations in NP prescriptive authority across states also influence long-term career mobility and retention; multistate licensure compacts may ease transitions but cannot fully circumvent differing legal constraints on prescribing controlled substances. For those weighing educational options, balancing program length with practical regulatory awareness is critical. Exploring the shortest DNP programs online can be a tactical choice, provided they integrate state-specific prescriptive authority nuances that affect employability and formulary access.
What education, certification, and licensure are required before NPs can prescribe?
Securing NP prescriptive authority requires navigating complex certification and licensure frameworks that differ drastically by state. Before prescribing medications, nurse practitioners must complete graduate-level clinical education-usually a master's or doctoral program-and obtain national certification to demonstrate competency in patient care management.
This certification aligns with licensure standards, which mandate an RN license plus an advanced practice registered nurse (APRN) endorsement explicitly authorizing prescribing privileges. These requirements reflect evolving state mandates that significantly impact prescribing scopes, especially for controlled substances.
For example, restricting nurse practitioners' rights to prescribe Schedule II medications remains rare but consequential; only Georgia and Oklahoma bar NPs from these prescriptions, confining authorities to Schedules III-V. Other states allow full Schedule II-V prescribing but impose conditions like DEA registration and continuing education focused on controlled substances.
These nuances in NP prescriptive authority education and licensure requirements in the United States influence both clinical autonomy and employment competitiveness, particularly in specialties like pain management and behavioral health. Working in states with restrictive prescribing policies demands extra oversight or alternative credentials, potentially limiting workflow efficiency. Employers prioritize candidates with unrestricted prescriptive privileges, associating this with compliance risk reduction and readiness to manage diverse patient needs.
Those seeking to pivot into or expand within nurse practitioner roles should carefully analyze these certification and licensure standards for nurse practitioners to prescribe medication to align educational investments with career goals. Prospective candidates exploring the path might also consider what is the easiest NP program to complete that still meets these regulatory criteria and practical demands, a topic discussed in depth at what is the easiest NP program.
How do controlled substance schedules affect what nurse practitioners can prescribe?
Nurse practitioners' prescribing authority is fundamentally constrained by federal controlled substance schedules and mandatory DEA registration, which directly affects their functional scope across specialties such as pain management and psychiatry. Despite state regulations on nurse practitioner prescribing schedules, failure to secure federal DEA registration effectively bars access to Schedule II-V medications, creating a significant operational bottleneck.
For instance, an NP in a rural clinic without DEA credentials cannot prescribe controlled pain medications, leading to delays as patients are referred to physicians. This not only impacts patient care timelines but also limits provider autonomy and workflow efficiency. From a workforce perspective, employers expect NPs to navigate controlled substance prescribing rules for nurse practitioners with thorough understanding of federal and state nuances.
Administrative requirements involve schedule-specific compliance, strict record-keeping, and timely renewals that must align with evolving regulations. NP programs that omit training on these protocols risk graduates entering the workforce underprepared for regulatory complexities, which can hinder employability in competitive specialty areas.
Students serious about entering roles requiring controlled medication management should prioritize a nurse practitioner school that integrates DEA registration processes and controlled substance prescribing rules into its curriculum. Preparing for this regulatory reality improves clinical flexibility and can influence long-term earnings and job placement.
Pragmatic decision-making involves weighing the added administrative steps against the expanded clinical role. For professionals evaluating NP programs, the inclusion of DEA compliance training is a critical factor in program selection to ensure readiness for real-world prescribing challenges. Explore detailed educational pathways in NP Programs at nurse practitioner school.
What are the key differences between NP and physician prescriptive authority?
Variations in prescriptive authority significantly influence the operational scope and career prospects for nurse practitioners compared to physicians. While physicians uniformly possess full prescriptive rights across all states-including controlled substances and off-label uses-NP prescriptive authority varies widely and remains contingent upon state legislation.
As of 2026, full practice authority allowing independent prescribing is granted in 29 states plus D.C. and two territories, rising from 24 states in 2020. Despite this legislative progress, many NPs remain bound by collaborative agreements or restricted formularies, limiting their ability to manage complex patient conditions autonomously. For example, an NP in a restrictive state must often obtain physician approval for controlled substance prescriptions, which can delay care delivery and reduce patient throughput.
- Physicians prescribe any medication without supervision; NPs often face formulary constraints and legal oversight depending on jurisdiction.
- Employers in full-practice states expect NPs to handle complex caseloads independently, whereas those in limited states may impose oversight or limit NP responsibilities.
- Choosing an NP program aligned with states granting full prescriptive authority strategically reduces post-licensure barriers and enhances professional flexibility.
These regulatory disparities directly affect workflow efficiency, compensation structures, and role definitions. NPs without full prescriptive rights often negotiate lower salaries and carry narrower clinical roles than physicians. Recognizing these distinctions is essential for prospective NP students evaluating educational pathways and long-term career viability within the healthcare workforce.
How do collaborative agreements and supervision impact NP prescribing rights?
Mandated collaborative agreements and supervised practice phases impose concrete limits on nurse practitioners' prescribing autonomy, shaping career trajectories in ways often underappreciated by prospective entrants. For instance, in states like New Jersey, a 2026 reform requires NPs to complete 5,000 hours of licensed clinical experience before independent prescribing is permitted.
Until this threshold is met, new NPs operate under joint protocols requiring physician co-signatures, which restricts their scope of practice and delays full clinical independence. These regulatory frameworks create distinct operational and employment dynamics:
- Primary care NPs in rural or underserved settings frequently encounter added administrative burdens and slower decision-making due to mandated oversight, impacting workflow efficiency and staffing flexibility.
- Conversely, psychiatric NPs in hospital environments with on-site physicians may navigate these restrictions more fluidly, benefiting from accessible supervision.
- Employers often prefer NPs who have completed supervised practice to mitigate compliance costs and oversight complexity.
For students entering NP programs, these real-world constraints translate into significant planning considerations. Securing supervising physicians, managing documentation requirements, and understanding jurisdiction-specific protocols are critical upfront investments. Without anticipating these factors, delays in obtaining full prescriptive authority can hinder upward mobility and salary growth. Consequently, evaluating NP programs requires rigorous scrutiny of these practical barriers alongside educational quality to ensure alignment with long-term professional goals.
How do online and campus NP programs prepare students for prescriptive authority?
Choosing between online and campus NP programs hinges on how well each addresses the complexities of state-specific prescribing regulations and clinical training realities. Campus-based programs offer direct, on-site supervision and clinical preceptors fluent in local prescriptive authority laws, easing navigation of mandates like Kentucky's four-year collaborative agreement requirement before independent prescribing.
This structure benefits students needing real-time policy updates and guided apprenticeship completion, which expedites licensure readiness. In contrast, online programs rely on remote simulations and tele-precepting, shifting responsibility to students to secure qualified, jurisdiction-aware clinical mentors. While flexible, this can delay hands-on experience with controlled substance approvals or non-scheduled drugs, extending the timeline to independent prescribing.
Considering workforce demand, ambulatory care employers typically expect immediate NP autonomy, whereas hospital settings often provide established oversight. Graduates aiming for rural primary care must prioritize programs with strong collaborative agreement training to avoid delays affecting earning potential and practice readiness.
What NP coursework and clinical experiences relate directly to prescribing safely?
Safe prescribing demands nurse practitioner students engage in pharmacology education that extends beyond theoretical knowledge to intensive clinical application. Core coursework should include drug mechanisms, interactions, and adverse effect monitoring, emphasizing controlled substances and evidence-based protocols.
Clinical rotations in settings like primary care or pain management clinics offer essential exposure to complex patient scenarios, such as managing polypharmacy in elderly patients or opioid therapy, where real-world judgment is tested. NP programs that fail to integrate substantial supervised prescribing experience leave graduates vulnerable to early-career prescribing errors and potential disciplinary consequences.
Employers increasingly seek candidates who demonstrate immediate, independent prescribing competence aligned with state-specific requirements, underscoring the value of programs that balance robust didactic content with clinically relevant hands-on training. The workforce also contends with continuing education demands, often mandated post-licensure, to maintain prescriptive authority.
This necessitates planning for ongoing pharmacology proficiency rather than viewing training as a finite phase. Programs prioritizing supervised dosage adjustments and monitoring prepare students for employer expectations more effectively. Limited clinical prescribing exposure compels new NPs to pursue supplementary mentorship or continuing education before full practice.
State regulatory variations influence the extent of required post-graduate pharmacology education. Prospective students evaluating NP programs should scrutinize both the intensity of pharmacology instruction and the availability of targeted clinical experiences, given the direct correlation between these factors and early-career prescribing outcomes.
How do prescriptive authority rules influence NP job roles, settings, and salaries?
State prescriptive authority significantly affects nurse practitioner (NP) roles, work environments, and compensation, with disparities rooted in regulatory autonomy. NPs authorized to prescribe independently in states with full authority typically earn 15-20% more than those in restricted states, reflecting higher employer demand and greater clinical flexibility. These NPs often work in primary or urgent care settings where streamlined workflows and fewer supervisory constraints enable increased patient volume and leadership opportunities.
Conversely, NPs in states with reduced prescriptive authority face administrative burdens due to mandated collaborative agreements with physicians. These require biannual documented meetings and retention of written records for at least a year post-agreement, reducing direct patient care time and limiting career mobility. For example, an NP in a rural hospital under such restrictions must dedicate recurring hours to compliance tasks, which employers factor into lower compensation and fewer advancement prospects.
Employers in autonomous states prioritize candidates capable of independent prescribing, influencing workforce composition and hiring competition. Prospective students and professionals evaluating NP programs should consider these regulatory environments' practical impacts on workload, earning potential, and clinical role scope to align educational choices with realistic career objectives.
How can NP students stay current on changing prescriptive authority laws and regulations?
Nurse practitioner students must actively integrate regulatory monitoring into their professional development to respond effectively to shifting prescriptive authority laws. The landscape is rapidly changing, with 29 states plus D.C. and two territories expected to permit full independent NP prescribing by 2026. Students aiming to practice in these jurisdictions face distinct requirements, they must demonstrate not only clinical competency but also detailed knowledge of independent prescribing protocols, which can vary significantly from states requiring collaborative agreements.
A practical example is an NP student targeting employment in a full-practice authority state. Such a student must align their education and licensure preparation to match local regulatory timelines and legislative changes. This includes utilizing state board communications, federal healthcare updates, and databases maintained by government agencies or specialized research institutions.
To stay ahead, students should adopt a multifaceted information strategy involving:
- State and federal regulatory updates from official healthcare bodies.
- Analyses from accredited academic institutions offering comprehensive NP programs.
- Active participation in professional NP association dialogues addressing implementation barriers and workforce expectations.
- Industry trend reports detailing how changes in prescriptive authority impact hiring and role scope.
This approach prepares students to anticipate policy shifts, strategically plan credentialing steps, and make informed academic choices that reflect the evolving workforce demand. These regulatory nuances directly influence an NP's capacity for timely care delivery and cost management in diverse clinical environments, underscoring the practical importance of continuous legislative engagement.
Other Things You Should Know About NP Programs
The structure and scheduling of clinical hours vary widely across NP programs, impacting your ability to balance work, life, and study. Programs that require fixed daytime clinical hours may not accommodate employed students well, leading to burnout or prolonged completion times. Prioritize programs offering flexible or evening/weekend clinical placements if you need to maintain employment throughout your study, as this flexibility strongly influences your ability to meet program requirements without compromising income or well-being.
Specialized NP programs (like family, psychiatric, or pediatric tracks) often provide targeted pharmacology and clinical experience aligned with their patient population, which better prepares you for prescriptive decisions within that specialty. Generalist tracks may offer broader exposure but less depth in prescribing practice for specific conditions, potentially requiring additional training post-graduation. If your goal includes working independently with robust prescriptive authority in a focused area, choosing a specialized program usually results in higher employer confidence and smoother transitions to prescribing roles.
While accreditation ensures that a program meets baseline educational standards, the quality and scope of clinical placements more directly affect your readiness for prescriptive authority. Programs with strong clinical networks provide diverse real-world prescribing scenarios and mentoring, which are critical for developing safe, competent prescribing habits. It is advisable to prioritize programs with established partnerships offering rich clinical experiences over programs with similar accreditation status but weaker clinical support, as this difference substantially impacts your practical training and employability.
Employers in high-demand or regulated settings often expect NPs to have completed programs with demonstrable clinical rigor in prescriptive authority, including documented training in controlled substances management. Choosing a program recognized for its integration of prescriptive laws and hands-on pharmacology improves your marketability and reduces onboarding time. When deciding which NP program to attend, prioritize those with outcomes showing strong employer alignment and graduate placement in prescriber roles, as this reduces barriers to employment and enhances career progression.
References
- California Schedule II Controlled Substances and Risk of Addiction https://nursingcecentral.com/lessons/california-schedule-ii-controlled-substances-and-risk-of-addicction/
- Prescriptive Authority vs Practice Authority: What's the Difference for Nurse Practitioners? https://www.singleaimhealth.com/article/prescriptive-authority-vs-practice-authority-whats-the-difference-for-nurse-practitioners
- State Practice Environment https://www.aanp.org/advocacy/state/state-practice-environment
- NP vs PA - What's the Difference? https://nursinglicensemap.com/resources/healthcare-careers/how-to-become-physicians-assistant-pa/pa-vs-np/
- Collaborative Agreement Between Physician and Nurse Practitioner Explained https://www.medicaldirectorco.com/collaborative-agreement-between-physician-and-nurse-practitioner-what-you-need-to-know/
- Nurse Practitioner Scope of Practice Laws by State https://www.bartonassociates.com/locum-tenens-resources/nurse-practitioner-scope-of-practice-laws/
- Changes in Controlled Substance Schedules https://lanp.enpnetwork.com/nurse-practitioner-news/58871-changes-in-controlled-substance-schedules-
- Nurse Practitioner vs Physician Assistant: Key Differences | USAHS https://www.usa.edu/blog/np-vs-pa/
- Top Online NP Programs in Massachusetts (Most Affordable) https://www.npschools.com/states/massachusetts
- Nurse Practitioner vs Doctor | Primary Care Differences https://tsiyyoncare.com/blog/nurse-practitioner-vs-doctor-primary-care/